
Review of Stroke Basics: Dissecting the ODEMSA Stroke/TIA Protocol
Overview
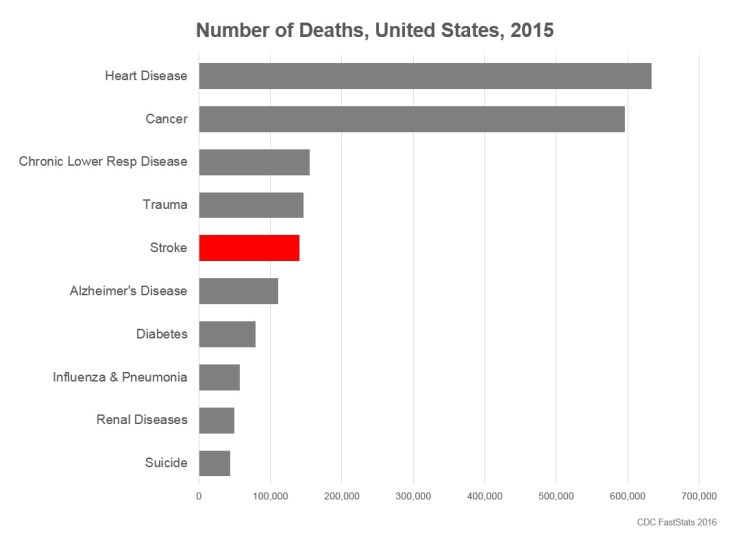
Stroke is the 5th leading cause of death in the United States, just behind trauma, with over 140,000 people dying from stroke in 2015 alone. There are multiple risk factors that contribute to increased risk of stroke, some of which can be mitigated with diet and lifestyle modification.
What is a Stroke?
A stroke occurs when there is an interruption of blood flow to the brain. This can occur by two major mechanisms, 1) blood vessel occlusion and 2) blood vessel rupture.
| Occlusive (Ischemic) Stroke | Hemorrhagic Stroke | |
| Pathophysiology | Occurs when the artery carrying blood to an area of the brain is blocked by a clot, cutting off or limiting downstream flow of blood and oxygen to areas of the brain. | Occurs when the artery carrying blood to an area of the brain ruptures or leaks, diverting blood and oxygen away from its intended target tissue. |
| Subtypes | Thrombotic – plaque/clot builds up within the vessel in the brain
Embolic – plaque/clot develops elsewhere in the body and travels to the brain |
Intracranial Hemorrhage (ICH)
Subarachnoid Hemorrhage (SAH) |
Considerations when taking the HPI
There are multiple pertinent questions to ask when taking a focused history of present illness (HPI) on a suspected stroke patient. We’ll review a few of the big ones:
What is the patient’s Last Known Well?
This is important for determining whether the patient is eligible for certain interventions like t-PA which have time windows.
Does the patient have a history of stroke or TIA?
This is relevant for many reasons. If the patient has had a stroke within the last 3 months, they are NOT a candidate for thrombolytic therapy (tPA). Additionally, history of prior stroke is a major risk factor for recurrence of stroke.
What other health conditions do they have?
Diseases like hypertension, diabetes and hypercholesterolemia increase one’s risk for stroke. Additionally, sometimes other diseases can cause the stroke itself, as is the case with atrial fibrillation. In atrial fibrillation, the blood in the chambers of the heart is not pumped out as fluidly as in healthy patients. This turbulent flow increases the risk of clot formation in the heart. These clots can then exit the chambers of the heart and travel up the carotid arteries causing an occlusive stroke. This phenomenon is called cardioembolic stroke. This is why patients with atrial fibrillation are prescribed blood thinners – to decrease their risk of this type of stroke.
Do they take any blood thinners?
Another contraindication to thrombolytic therapy (tPA) is if the patient has a known reason to bleed. So if platelets are <100,000, the patient cannot receive tPA. Likewise, blood thinners like Warfarin or Xarelto, also make patients prone to bleeding. If the patient is on a blood thinner by history or there is evidence of their use on labs (e.g. INR>1.7), tPA cannot be given, which changes the plan of care by the hospital Stroke Team.
Have they suffered head trauma?
As with a history of stroke, patients who have suffered head trauma within the last 3 months are also NOT candidates for thrombolytic therapy (tPA).
Please review the ODEMSA protocol for additional pertinent HPI elements.
Note their signs & symptoms
Symptoms of stroke (the patient’s subjective report of what he/she is experiencing) can range from subtle to obvious. The patient may tell you “I can’t move my left side,” or they may only offer “I just don’t feel right.” Similarly, signs (your physical exam findings) can also range from subtle to obvious. Slurred speech, garbled speech, slow speech and confused speech are all different signs and potentially different types of strokes. Don’t just document and report “abnormal speech” – be specific.
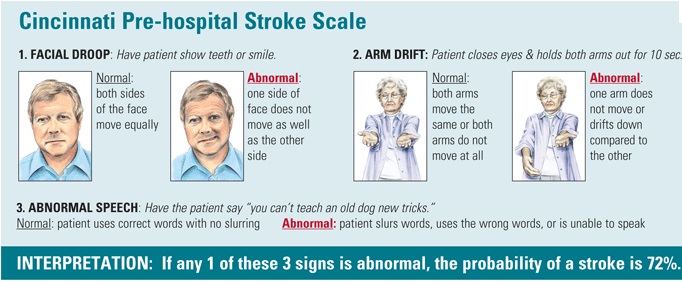
Fortunately most EMS systems have adopted validated prehospital stroke assessment tools for use in the field. ODEMSA is no exception. Providers should perform a Cincinnati Prehospital Stroke Scale (CPSS) or a FAST assessment on all suspected stroke patients. If either of these initial screening tools are positive, providers should then conduct a VAN assessment. Please review the ODEMSA Stroke/TIA protocol if you are unfamiliar with CPSS or FAST.

Other consideration for the Differential Diagnosis
Whenever you encounter a patient with a neurological complaint, whether limb paralysis or confusion, it’s important to consider and evaluate for stroke; however, not all neurological deficits are due to stroke. For example, the standard of care in management of possible stroke patients is to check a glucose level quickly and early in care. Hypoglycemia can present as a focal neurological deficit in some patients. Additionally, a subset of seizures called Todd’s paralysis can cause unilateral weakness that looks just like a stroke. These subtleties can be difficult to tease out in a fully-equipped Emergency Department, not to mention the back of an ambulance, so follow your protocols and consider use of the Unconscious/Syncope/AMS patient care protocols as well.
Considerations in Hospital Selection
The medical directors of the ODEMSA region have created triage and transport guidelines to direct providers where to take stroke patients under certain circumstances. Please refer to the 2018 ODEMSA Stroke Triage Plan for guidance on where to take your patient and when.
To learn more about VAN and large vessel occlusions (LVOs), please review the educational material located at LEARN VAN.
